Clinical history:
Non-consanguineous couple (30 yrs, male and 29 yrs, female) married for 2 years were referred for preconception genetic counseling in view of male partner being clinically diagnosed with Foveal hypoplasia Nystagmus.
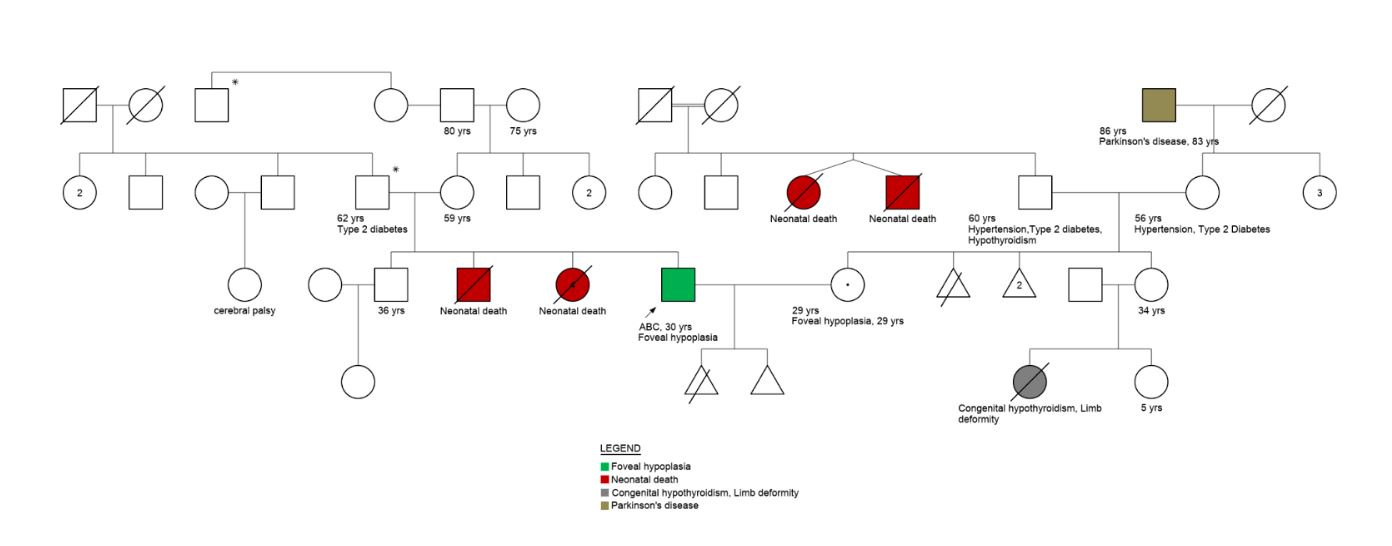
PEDIGREE
Pretest GC:
OBSTETRIC HISTORY:
G1: Conceived naturally after 1 year of marriage. At 6 weeks fetal cardiac activity was absent. The couple opted for medical termination of pregnancy.
G2: conceived naturally. NT scan at 12 weeks was normal. At 12 weeks of gestation spontaneous miscarriage was observed in view of cervical incompetence. D&C was done.
Family history significant for multiple neonatal deaths, cerebral palsy, multiple spontaneous miscarriages.
Genetic Tests and results:
After pre-test GC, the genetic counselor advised to take these tests:
1. Couple Karyotype- normal
2. SMA (SMN deletion/duplication analysis)
3. Hb electrophoresis testing for both the partners
4. DMD and Fragile X testing for female partner- normal
5. Couple carrier screening
- Pathogenic homozygous mutation SLC38A8 c.794A>G (p.Tyr186Ter) associated with Foveal hypoplasia 2 (OMIM *615585)
- Heterozygous mutation c.558C>G (p.Tyr265Cys) SLC38A8 gene associated with Foveal hypoplasia 2 (OMIM *615585). This genetic changes are classified as Variant of uncertain significance (VOUS)
Implications for Results:
- When both parents are carriers for disease-causing (pathogenic) genetic changes, prenatal genetic testing or preimplantation genetic testing can be offered.
- Here the husband has two copies of genetic mutation while the wife has a variant in the same gene though currently we have limited information regarding its association with the disease.
- Since male partner is affected with Foveal hypoplasia and has homozygous pathogenic variants, all the future children will inherit one mutation. Due to the uncertainty of the clinical significance of the VUS in the female partner, we cannot predict if the child inherits the VUS with a variant (50%) will be affected or remain a carrier.
- In such cases, as per guidelines preimplantation or prenatal genetic testing is not recommended. The ASHG (the American Society of Human Genetics) guidelines, it is not recommended that Variants of Uncertain Significance be used for clinical decision making.
Psychological impact:
Identifying variants of uncertain significance in prenatal or preconception settings can be emotionally challenging, increase anxiety and uncertainty planning or during the pregnancy. Couples may also feel differently about the risk associated and the further course of action. Genetic counseling should focus on addressing these emotional reactions with the couple.
Conclusion:
Genetic counselors must help families navigate the challenges variants of uncertain significance bring in a prenatal or preconception setting such as risk assessment, genetic testing options and adapting to risk and uncertainty.